
Aortic Valve Replacement (AVR)
Background
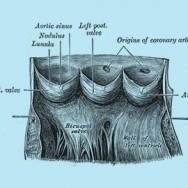
The aortic valve controls blood flow between the left ventricle and the aorta, the artery that delivers oxygen-rich blood to the body. There are two main problems that can occur with the aortic valve: it can become hardened and narrowed (stenosis), or it can leak (regurgitation). The most common problem in the elderly is called age-related calcific degeneration, where the gradual buildup of calcium causes the valve to narrow. In younger patients a bicuspid valve (two leaflets instead of three) is a common cause. Other causes include rheumatic heart disease and infection (endocarditis). Symptoms of aortic valve disease may include light-headedness, chest pain, shortness of breath and fatigue.
About the surgery
Aortic valve replacement is the most effective method of treating severe aortic valve disease. It involves removing the diseased valve and replacing it with an artificial valve. There are two types of artificial valves: biological (tissue) valves (commonly made out of pig tissue (porcine) or cow tissue (bovine), and mechanical valves (made out of carbon fibre). Mechanical valves are very durable, and rarely fail. However they require life long blood thinners (anticoagulation) such as warfarin, which increase the risk of bleeding and need regular monitoring. On the other hand, biological valves do not require blood thinners, but do not last as long as mechanical valves. The average time a biological valve lasts is around 15-20 years, and the patient may require another operation after this. This is a complex decision that ultimately the patient must make, and they should discuss the differences with their surgeon.
In the procedure, the sternum (breast) bone is divided to access the heart. The patient is then put on the heart-lung machine, the heart stopped, and then the aortic valve is replaced. At this time the surgeon may also perform other procedures if needed, such as coronary artery bypass grafting, to avoid the patient needing another operation.
Recovery period
For a while after the surgery, patients may feel worse than they did before surgery. This is normal and is usually related to the trauma of surgery, not necessarily to the functioning of the heart. Patients usually stay in the intensive care unit for 1 – 2 days for monitoring, and then in the nursing unit for 4 – 5 days. Two to three tubes stay in the chest to drain fluid from around the heart, which are usually removed 1 – 3 days after the surgery. Full recovery usually takes about 2 months. Most patients are able to drive in about 3 to 8 weeks after surgery. Your surgeon will provide specific guidelines for your recovery and return to work.
Risks of the surgery
As with all surgery, aortic valve replacement is associated with some risks. Your surgeon will calculate these risks specific to you, and discuss them with you. In the short-term after the operation these include wound infection, bleeding, kidney injury, stroke, heart attack, arrhythmias and pacemaker implantation, and possibly death. In the long-term the artificial valve may fail, and another operation may be required.
For more information please visit:
Cleveland Clinic Aortic Valve Surgery
All patients should consult their cardiothoracic surgeon for specific information about their medical condition and surgery.