
Mitral Valve Surgery
Background
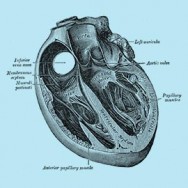
The mitral valve controls blood flow between the chambers on the left side of the heart, which pumps oxygenated blood to the body. There are two main problems that can occur with the mitral valve: it can become too narrow (stenosis), or it can leak (regurgitation). Abnormal blood flow through the valve will then cause the heart to work harder, and eventually lead to heart failure. Symptoms of this include shortness of breath, light-headedness, fatigue, chest pain or palpitations.
About the surgery
Depending on the type of mitral valve disease, the valve can either be repaired or replaced with an artificial prosthesis. Repair is preferred over replacement since it provides better long-term survival, better preservation of heart function, lower risk of complications, and eliminates the need for long-term use of blood thinners (anticoagulants). Repair can be performed in most patient with regurgitant mitral valves, and some with stenotic mitral valves. There are a number of ways of repairing the mitral valve, and some example include sewing a ring around the outside of the valve (called ring annuloplasty), removing some of the leaky parts of the valve leaflets (called resection), or replacing some of the cords that connect to the valve (called neo-chordae).
If the mitral valve does need to be replaced, then there are two types of artificial valves: biological (tissue) valves (commonly made out of pig tissue (porcine) or cow tissue (bovine)), and mechanical valves (made out of carbon fibre). Mechanical valves are very durable, and rarely fail. However they require life long blood thinners (anticoagulation) such as warfarin, which increase the risk of bleeding and need regular monitoring. On the other hand, biological valves do not require blood thinners, but do not last as long as mechanical valves. The average time a biological valve lasts is around 15-20 years, and the patient may require another operation after this. This is a complex decision that ultimately the patient must make, and they should discuss the differences with their surgeon.
Recovery period
Patients usually stay in the intensive care unit for 1 – 2 days for monitoring, and then in the nursing unit for 4 – 5 days. Two to three tubes stay in the chest to drain fluid from around the heart, which are usually removed 1 – 3 days after the surgery. Full recovery usually takes about 2 months. Most patients are able to drive in about 3 to 8 weeks after surgery. Your surgeon will provide specific guidelines for your recovery and return to work.
Risks of the surgery
As with all surgery, mitral valve repair and replacement are associated with some risks. Your surgeon will calculate these risks specific to you, and discuss them with you. In the short-term after the operation these include wound infection, bleeding, kidney injury, stroke, heart attack, arrhythmias and pacemaker implantation, and possibly death. If the mitral valve was replaced, then in the long-term the artificial valve may fail, and another operation may be required.
For more information please visit:
Cleveland Clinic Mitral Valve Repair
Medline Plus Mitral Valve Surgery
All patients should consult their cardiothoracic surgeon for specific information about their medical condition and surgery.